
What is hereditary Bowel Cancer?
Bowel cancer (also known as colorectal cancer) is the fourth most common cancer in the UK. Unfortunately, 1 in 18 women (6%) and 1 in 15 men (7%) will develop bowel cancer during their lifetime, with more than 40% being diagnosed over the age of 75.

Most bowel cancer occurs by chance, however 2-5% of bowel cancer is inherited and up to 30% is familial. In some families’ stomach, womb (endometrial or uterine) and ovarian cancer can also be genetically related to bowel cancer. In families where bowel cancer is hereditary it may be possible to find the genetic change (pathogenic variant) which is responsible for the cancers. This allows appropriate cancer screening and risk-reducing options to be offered to the family.
What are genes?
Genes are the body’s instructions and they determine how the body develops and is maintained. Some genes prevent cancer developing: if there is a pathogenic variant in one of these cancer genes, then the gene doesn’t work correctly and this causes an increased risk of cancer. Pathogenic variants in at least 19 genes can cause an increased risk of bowel cancer and other cancers. However, we know that there are other genes which are also associated with bowel cancer and research is attempting to understand these other genes.

How are pathogenic variants inherited?
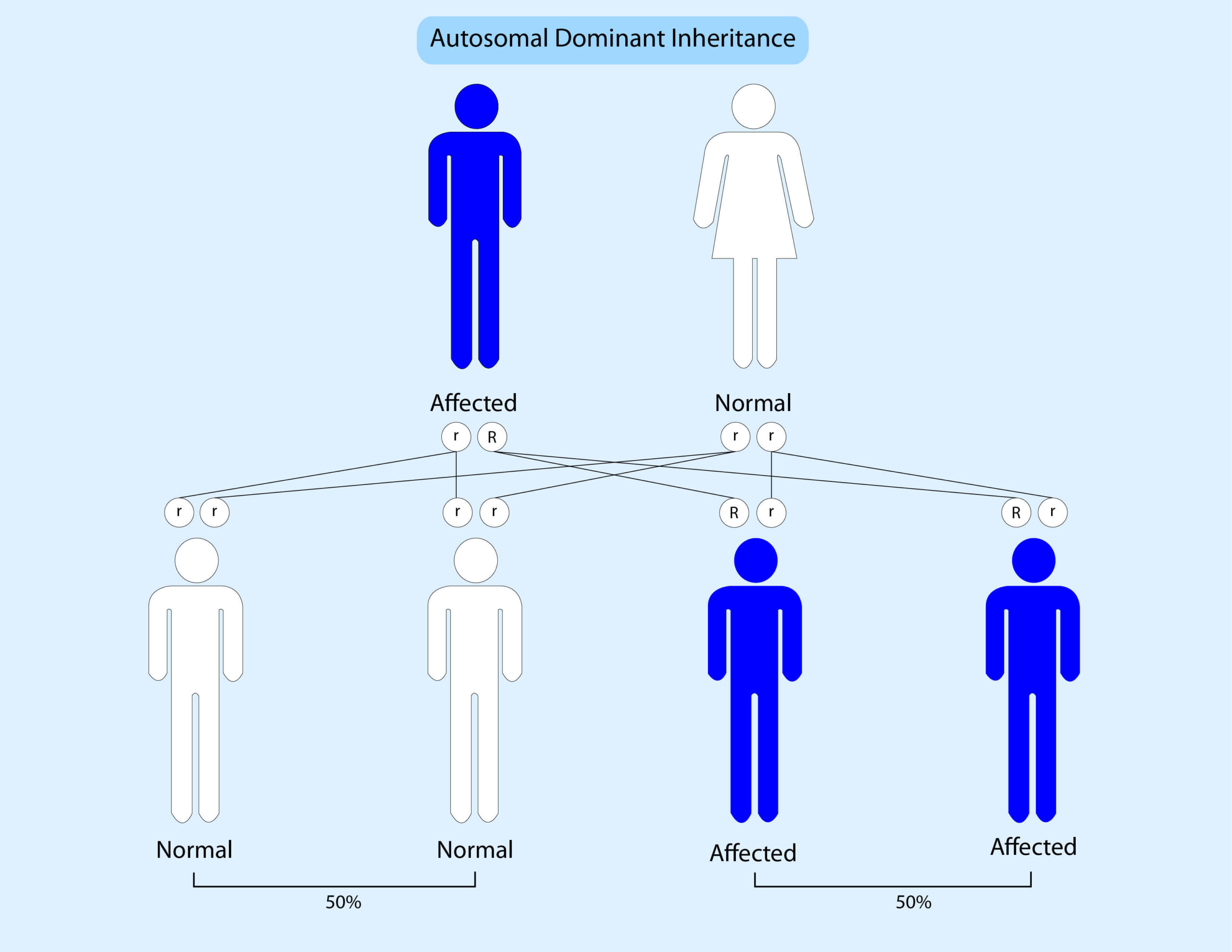
Genes come in pairs; we get one copy from our mother and one copy from our father. Currently most inherited bowel cancer syndromes are inherited in a dominant pattern. This means that if someone has a mutation in one copy of a gene then there is a 50% (1 in 2) chance that they will pass this onto their children. The diagram below shows this:
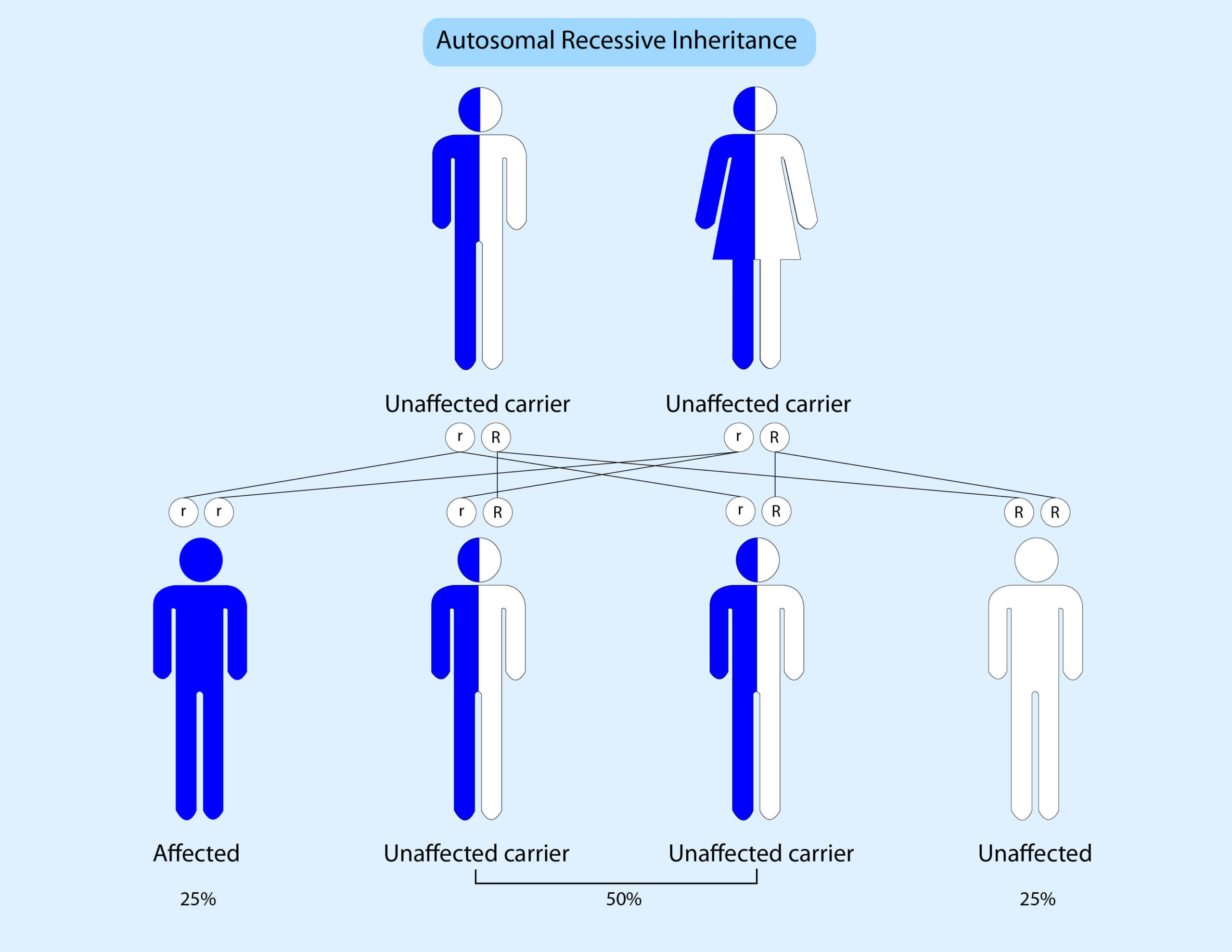
Occasionally an increased risk to bowel cancer can be inherited in an autosomal recessive pattern. This means that someone must inherit a pathogenic variant from their mother AND father to be affected. The diagram below illustrates this:
What screening would my relatives need?
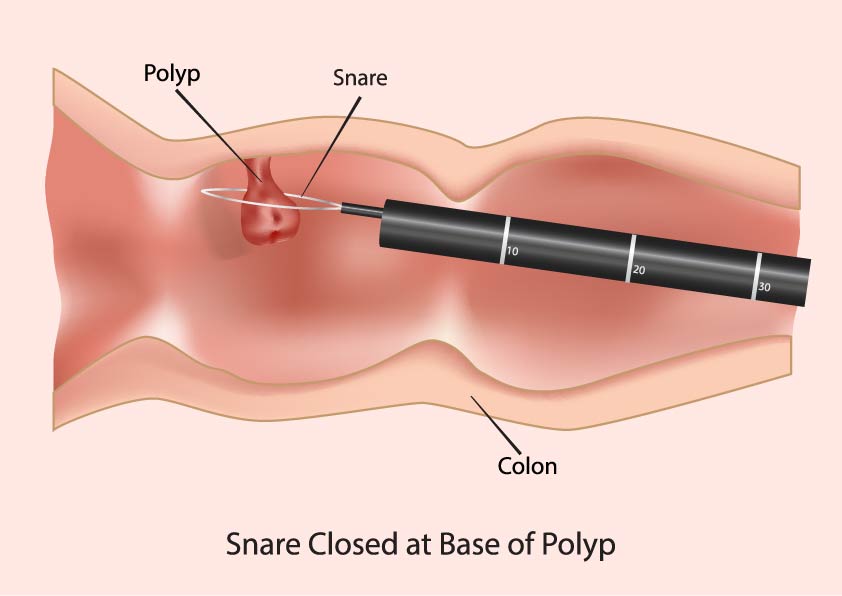
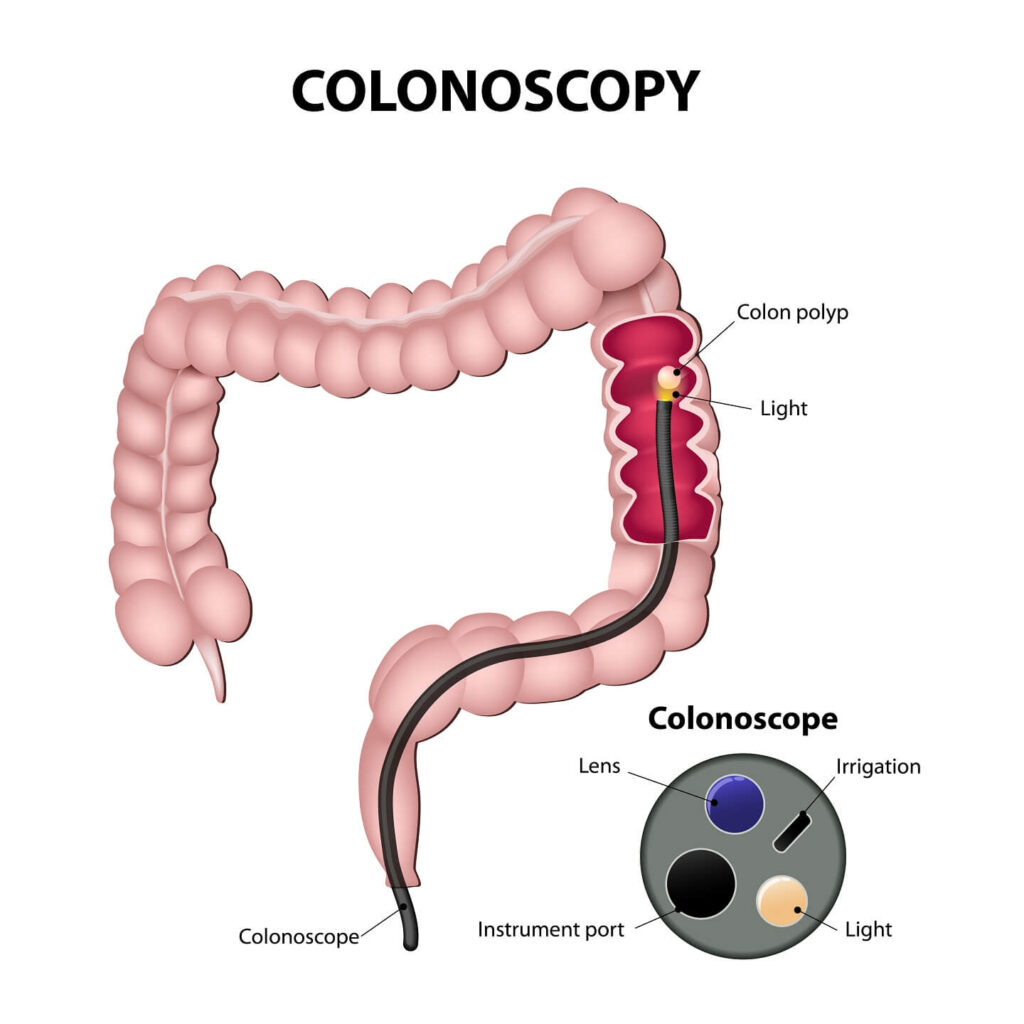
When someone has an increased risk of bowel cancer it is usual for them to have colonoscopies. A colonoscopy is when a flexible telescope is inserted into the anus to examine the entire bowel (rectum and colon). If any polyps are found these can usually be removed to prevent them developing into cancer. The frequency of colonoscopy will depend on which gene variant is found.
Screening for other cancers may also be needed and will be discussed if necessary. Aspirin has been shown to lower the risk of bowel cancer in some circumstances and is currently recommended for LS carriers.
Risk-reducing surgery
In some situations, people may wish to consider risk- reducing surgery. This is dependent on the condition. In Lynch syndrome women have an increased risk of womb and ovarian cancer and may therefore consider hysterectomy and removal of the ovaries.
In some conditions, people may also consider colectomy (removal of the colon).
Bowel awareness
It is important for everyone to be bowel aware and inform their doctor if they notice any signs that they are concerned about.
The symptoms of bowel (colorectal) cancer in men and women can include:
- bleeding from the back passage (rectum) or blood in your poo
- a change in your normal bowel habit, such as looser poo, pooing more often or constipation
- a lump that your doctor can feel in your back passage or tummy (abdomen), more commonly on the right side
- a feeling of needing to strain in your back passage (as if you need to poo), even after opening your bowels
- losing weight
- pain in your abdomen or back passage
- tiredness and breathlessness caused by a lower than normal level of red blood cells (anaemia)
Further information and support can be found at:
www.corecharity.org.uk 020 7486 0341
www.researchuk.org 0808 800 4040
www.macmillian.org.uk 0808 808 0000
www.bowelcanceruk.org.uk 0800 8403540
![]()
![]()
![]()