
Breast Cancer Genetics Testing
Hereditary Breast Cancer
What is hereditary breast Cancer?
Breast cancer is the most common cancer in the UK. Unfortunately, 1 in 8 women (13%) will develop breast cancer during their lifetime; with 80% being diagnosed after the age of 50. 1 in 868 men will also be diagnosed with breast cancer. Most breast cancer occurs by chance, however approximately 5-10% is hereditary and in some families ovarian cancer can be genetically related to breast cancer. In families where breast cancer is hereditary it may be possible to find the genetic change (pathogenic variant) which is responsible for the cancer. This allows for appropriate cancer screening and risk-reducing options.
Who is at risk of hereditary breast cancer?
Women who have been diagnosed with breast cancer and meet one or more of the following criteria have an increased risk of hereditary cancer:
- Breast cancer diagnosed before the age of 45
- Bilateral breast cancer (cancer in both breasts)
- Triple negative breast cancer (ER negative, PR negative, HER2/neu negative)
- Ovarian cancer
- Several close relatives with breast cancer or prostate cancer
- One or more close relatives with male breast cancer or ovarian cancer
- Jewish ancestry
It is important to be aware that hereditary breast cancer can be present on either the maternal (mother’s) or paternal (father’s) side of the family.
What are genes?
Genes are the body’s instructions and they determine how the body develops and is maintained. Some genes prevent cancer developing: if there is a pathogenic variant in one of these cancer genes, then the gene doesn’t work correctly and this causes an increased risk of cancer. Pathogenic variants in at least 12 genes can cause an increased risk of breast cancer and other cancers. However, we know that there are other genes which are also associated with breast cancer and research is attempting to understand these other genes.

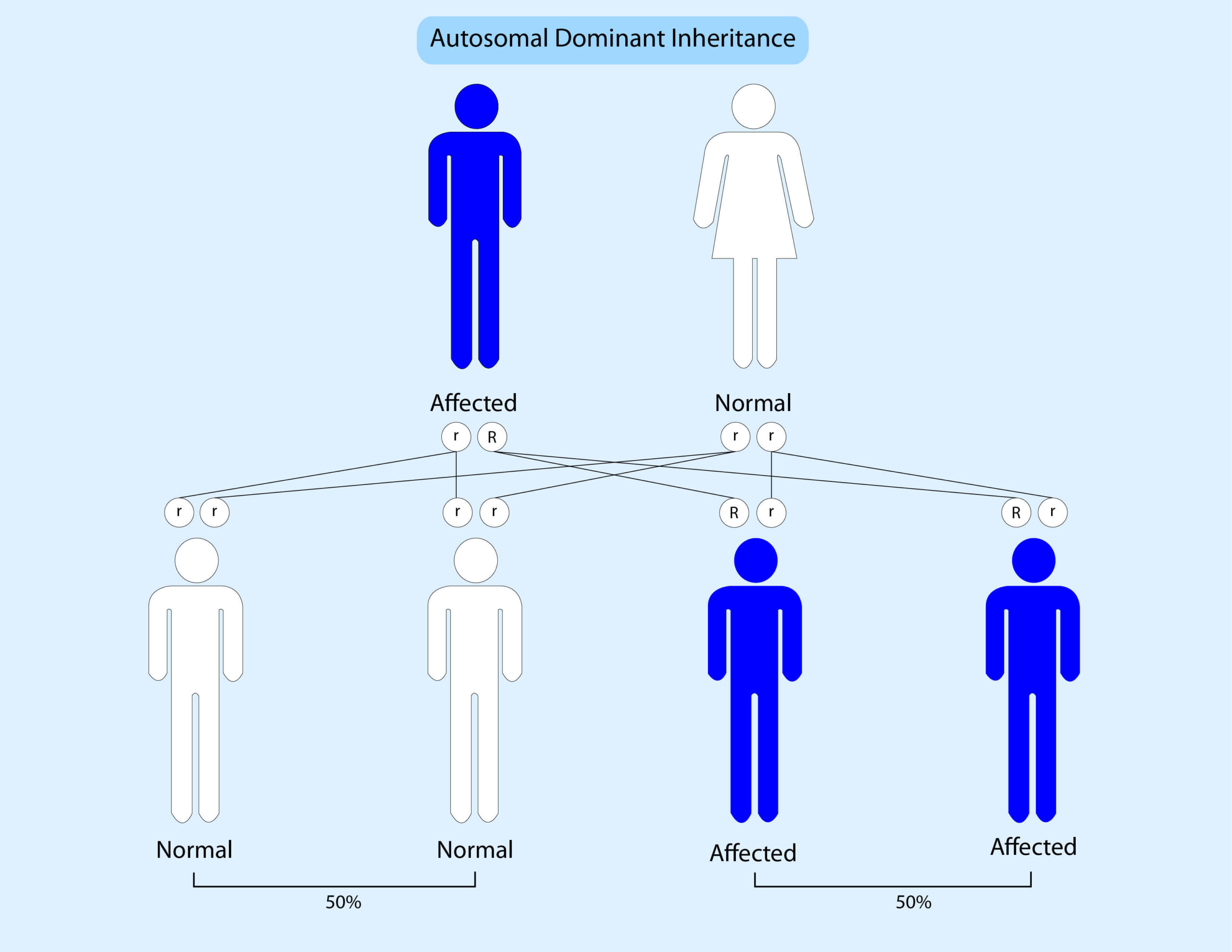
How are pathogenic variants inherited?
Genes come in pairs; we get one copy from our mother and one copy from our father. At present all known breast cancer syndromes are inherited in a dominant pattern. This means that if someone has a pathogenic variant in one copy of a gene then there is a 50% (1 in 2) chance that they will pass this onto their children. The risk of breast cancer can be inherited from either side of the family.
The diagram below illustrates this:
What genes are tested?
Breast Cancer Genetic testing looks at 12 specific genes which cause an increased risk of breast cancer. These genes are: ATM, BARD1, BRCA1, BRCA2, CDH1, CHEK2, PALB2, RAD51C, RAD51D, PTEN, STK11, TP53.
How does the test work?
Genetic testing is performed on a blood or saliva sample and it usually takes 2 weeks to obtain the results. The test looks at the genes in detail and also looks for large deletions (missing parts) and duplications (extra parts) of the genes. However, no test is 100% accurate and it is possible that someone could have a genetic pathogenic variant which is not detected by this test.
What will the test show?
There are 3 possible results:
- A pathogenic variant is found in one of the genes which is known to increase the risk of breast cancer. This may impact your chemotherapy and/or surgery. Future cancer screening and/or risk-reducing techniques may also be recommended.
- A variant of uncertain significance or VUS is found, but whether or not this is the definite cause of cancer is unknown. Your cancer treatment will remain unchanged and cancer screening will be based on your family history.
- No pathogenic variant is found. Your cancer treatment will remain unchanged and cancer screening will be based on your family history.
What does it mean if I have a pathogenic variant?
If you have a pathogenic variant this will explain why you developed breast cancer and unfortunately means that you may have increased cancer risks in the future. Your exact risk(s) will depend on which gene pathogenic variant has been found. Extra screening and/or risk- reducing strategies will be discussed. It will also be possible to offer predictive testing to other people in your family to see if they also have the pathogenic variant.
Surgery: some women who have been diagnosed with breast cancer and are shown to have a pathogenic variant may choose to have a bilateral mastectomy as their primary surgery or to consider this in future.
Additionally, women with a BRCA pathogenic variant may consider bilateral salphingo-oophorectomy (removal of the ovaries and tubes) in future although this would be a preventative option and therefore not urgent.
Screening: When someone has an increased risk of breast cancer it is usual for them to have screening using mammography and often breast MRI scans. The frequency and timing of mammography will depend on which genetic pathogenic variant is found. Screening for other cancers may also be needed and will be discussed if necessary.
Hereditary Breast Cancer Conditions
Hereditary Breast and Ovarian Cancer (HBOC): Pathogenic variants in BRCA1 & BRCA2 cause hereditary breast and ovarian cancer. In the general population 0.4% of non-Jewish people and 2% of Ashkenazi Jewish people will have a BRCA pathogenic variant. The estimated cancer risks associated with BRCA pathogenic variants vary; however, BRCA1 pathogenic variants are estimated to cause up to an 85% lifetime risk of breast cancer and a 40-60% risk of ovarian cancer. Men with BRCA1 pathogenic variants may have a 1-2% risk of male breast cancer and an increased risk of prostate cancer.
Women with BRCA2 pathogenic variants have up to a 90% lifetime risk of breast cancer and up to a 26% risk of ovarian cancer. Men with BRCA2 pathogenic variants have a 5-10% lifetime risk of developing breast cancer, and approximately a 20% risk of prostate cancer. Individuals with BRCA2 pathogenic variants also have an increased risk of pancreatic cancer and possibly other cancers.
Women with BRCA gene pathogenic variants should have annual breast screening from 30 years including mammograms and breast MRI. Ovarian cancer screening has not been shown to detect cancer sufficiently early to save lives and therefore some women may consider risk-reducing surgery. Men may benefit from prostate cancer screening with PSA testing. Occasionally, a baby will inherit two BRCA2 pathogenic variants and will therefore have the congenital condition known as Fanconi Anaemia.
PTEN Hamartoma Tumour Syndrome / Cowden syndrome: Cowden syndrome causes bowel polyps, benign skin lesions, benign breast disease, autism and other features. Individuals with Cowden syndrome have an increased risk of bowel, breast, kidney, thyroid and womb cancers as well as an increased risk of melanoma. Colonoscopy as well as mammograms, renal MRI, skin examination and thyroid ultrasounds will be recommended. Risk reducing surgery may be considered.
Peutz Jeghers Syndrome (PJS): PJS causes polyps in the large and small bowel, as well as ovarian tumours and abnormal colouring of the skin, particularly on the lips in childhood. PJS causes an increased risk of bowel, breast, pancreatic and other cancers. Mammography, colonoscopy and other cancer screening tests will be recommended.
Hereditary diffuse Gastric Cancer (HDGC): HDGC causes a high risk of diffuse stomach and lobular breast cancer as well as a probable increased risk of bowel cancer. Endoscopy, possible gastrectomy (removal of stomach), breast and bowel screening will be discussed. People should also be screened for Helicobacter Pylori (a type of infection) and treated if necessary. Individuals with HDGC should be treated at a centre with expertise in the condition.
Li Fraumeni Syndrome (LFS): Li Fraumeni syndrome is a relatively rare condition which causes a high risk of cancer in childhood and adulthood: approximately 1 in 5000 to 1 in 20000, people will have LFS. Li Fraumeni syndrome causes an increased risk of sarcomas, brain tumours, breast cancer, adrenal cortical carcinomas and other cancers. Individuals with TP53 pathogenic variants have a 50% risk of developing some type of cancer by age 30 and a lifetime risk of up to 90%. Breast screening with MRI will be recommended. Individuals are also advised to avoid radiation as they have an increased radiation sensitivity.
ATM associated breast cancer: Approximately 1 in 200 people (0.5%) will carry a pathogenic variant in the ATM gene. Individuals with a pathogenic variant in the ATM gene have a moderately increased risk of breast cancer, as well as an increased risk of radiation-sensitivity. Increased breast screening is recommended.
Rarely a baby may inherit an ATM pathogenic variant from their mother AND their father, in which case they will have the congenital condition called Ataxia- Telangiectasia (AT). AT causes uncontrollable movements (ataxia), immune defects, and an increased risk of leukaemia and lymphoma.
CHEK2: Pathogenic variants in the CHEK2 gene are found in 4% of families with hereditary breast cancer and cause a moderately increased risk of breast cancer as well as a possibly increased risk of bowel cancer. Very rarely individuals have been shown to carry 2 pathogenic variants in the CHEK2 gene which seems to cause a higher risk of breast cancer. Increased breast screening, and in some situations, bowel screening will be recommended.
PALB2: Pathogenic variants in PALB2 have been shown to cause an increased risk of breast cancer. The risk is estimated to be approximately 35% although the risk is greater if there is a strong family history of breast cancer (up to 57%) and our knowledge of PALB2 is rapidly increasing. Increased breast screening with mammography and MRI is recommended. PALB2 also causes an increased risk of pancreatic and ovarian cancer. Occasionally, a baby will inherit two 2 PALB2 pathogenic variants and will therefore have the congenital condition known as Fanconi Anaemia.
RAD51C and RAD51D: Pathogenic variants in these genes are known to cause a moderately increased risk of both breast and ovarian cancer. The increased risk is particularly noticeable for triple negative breast cancer. Increased breast screening will be recommended, and some women may consider have their ovaries removed post menopause.
BARD1: Information about this gene is still emerging. However pathogenic variants have been shown to cause a moderately increased risk of breast and particularly triple negative breast, cancer and therefore increased breast screening is recommended.
Further information and support can be found at:
www.breastcancergenetics.co.uk
www.menagainstbreastcancer.org
Our knowledge of cancer genetics is rapidly growing, and the information given summarises this to date.
Have a question for us?
Contact us
Don’t hesitate to contact us to find out more about genetic testing and consultations
Genetic Experts UK
Email: info@geneticexperts.co.uk
Phone: 0333 339 2680
This site is protected by reCAPTCHA and the Privacy Policy and Terms of Service apply.
Copyright © 2021 Genetic Experts UK – All Rights Reserved.
![]()
![]()
![]()
Copyright © 2021 Genetic Experts UK – All Rights Reserved.
Website created by Col-Tech Group